The United States has the best health care that money can buy, provided one has the money to buy it. Jill Quadagno’s “One Nation Uninsured” answers the question “Why the U.S. has no national health insurance.” It’s a brisk, engaging read that neatly summarizes how 90 years of failed reform efforts have entrenched the powerful interests that profit from the system.
The most prominent early opponents of a national health service were the doctors themselves. Their lobby, the American Medical Association, fought against “socialized medicine” out of fear that it would lead doctors to lose their sovereignty to bureaucrats basing decisions on budgetary needs rather than medical needs. Allied with southern politicians who feared that a federal health system would force racial integration of hospitals, these forces successfully kept national health care out of Roosevelt’s original Social Security legislation. They favored market solutions like Blue Cross and commercial insurance. A new business was created, resulting in a more powerful lobby.
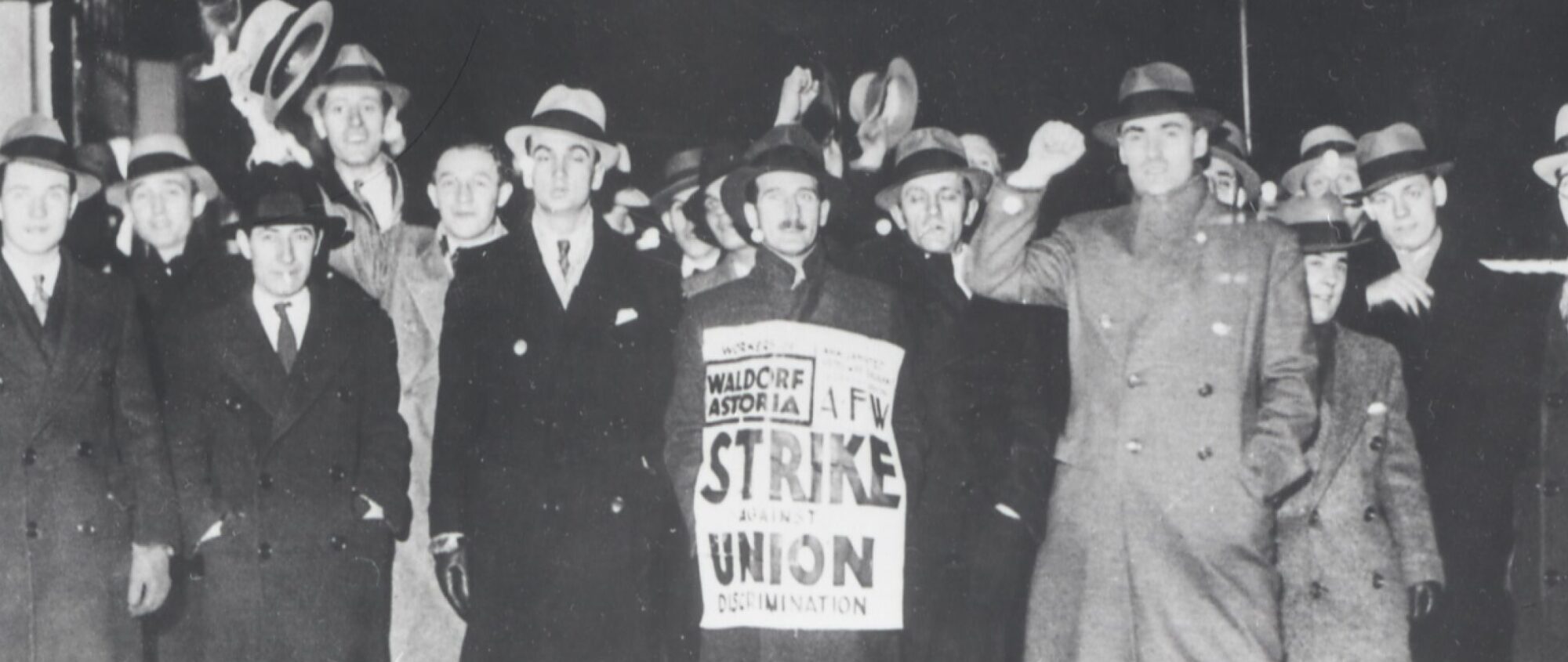
The trade union leaders of the time, many of whom were social democratic in their outlook, reluctantly shifted their efforts at creating a social safety net to the bargaining table, winning employer-sponsored health care plans. Some unions – notably Sidney Hillman’s Amalgamated Clothing Workers – created their own networks of health care clinics, socialized medicine in miniature. Wartime government policies that encouraged fringe benefits over wage increases greatly expanded the private welfare state so that by the 1950’s, most large employers (including non-union firms that aimed to remain non-union) provided health care benefits.
Trade unions continued to push for a government solution to health care, but by the 1960’s they narrowed their focus to the proverbial “camel’s nose under the tent,” health insurance for the nation’s elderly. The Medicare program that the coalition of labor and seniors won had several unintended consequences. One was that with senior citizens covered through the program, and most working families fully covered by an employer’s plan, few voters clamored for a universal national health care system for the next few decades. Another consequence, happily, was the racial integration of most hospitals, under threat of being denied Medicare funding.
A regrettable consequence of Medicare was rampant inflation of cost of health care. Doctors and hospitals provided comprehensive care for senior citizens, ordering tests, procedures and drugs that they might not have before there was guaranteed funding, which was a boon not only to the health of senior citizens but to the corporate bottom line of the for-profit hospitals and insurance companies that joined the market for health care services. The cost of Medicare skyrocketed, until government efforts to control costs caused insurance companies to simply pass on the costs to employers in the form of higher premiums for their employees. Companies responded in turn by cutting benefits, introducing co-pays and turning to health maintenance organizations to control costs by denying care. The doctors’ worst fear, losing sovereignty over medical decisions, was realized through the insurance companies that they were responsible for creating.
This brings us to our current circle of hell, where an employer’s threat to cut benefits leaves many unions close to helpless in contract negotiations, where people with the dreaded “pre-existing condition” are denied meaningful coverage and where the existence (or non-existence) of national health care or employer-sponsored insurance goes a long way towards determining a company’s competitiveness in the global economy.
This January, I’ll be taking an elective class with Dean Robinson that will be exploring the United States’ lack of a national health service and its impact on our health, wealth and democracy. Quadagno’s “One Nation Uninsured” is the first book assigned. Others are Kawachi and Kennedy’s “Health of Nations: Why Inequality Is harmful to Your Health” and Sered and Fernandopulle’s “Uninsured in America.” For my paper, I will be taking a look at some trade union health clinics, particularly the Amalgamated’s (now UNITE HERE) and the NY Hotel Trades Council’s, which was inspired by Hillman’s example. These socialized medicine-in-miniature not only provide comprehensive health services, but they keep costs so low that employers actually offer up concessions in order to take part.
The lesson here, I think, is that while we might succeed in creating a single-payer health care system like Canada’s (particularly as health care becomes more of a crisis), inflation and price-gouging will be crippling until we take the profit out of the system and nationalize health care services to serve the interests of the people, not the corporations.